Women’s Groups Leading the Way Towards Self-Reliance in Mali
August 20, 2019 | 4 Minute ReadRural women’s groups in Mali are proving that community health systems get stronger when national-level interventions are paired with community-level capacity building to make communities self-reliant.
On a recent visit to a rural village in Dioila district, part of the Koulikoro region in Mali, I met with the local women’s group to discuss how to promote family planning and reproductive health (FP/RH) and how to increase access to these services in their community. There, surrounded by more than 100 volunteers who dedicate their time to advocate for improved FP/RH access and services, a persistent thought came to my mind: rural women’s groups like this one are fundamental to a community’s self-reliance.
As global development professionals, we need to understand how the community self-reliance process works and how to replicate it in different settings when possible. So, I asked myself a not-so-simple question: Why are women’s groups so successful, and what does that mean for future efforts to improve health systems at every level?
Establishing a System for Women, by Women
Community-based groups are a frequent intervention point in global health projects given their ability to yield high impact results. In Mali, women’s groups have existed as a response to historically weak central and regional government systems, which often leave communities without support. To address different issues within communities, grassroots groups develop to advocate for issues like women’s and childhood education, FP/RH services, and local governance.
Although these groups have existed in Malian communities for some time, project and donor support enables them to effectively provide FP/RH guidance and resources to their neighbors. For instance, donor support helped community midwives serve as the critical link between community health centers and the health system. They now have access to the resources they need and regularly meet with technical staff at local hospitals to discuss challenges and receive training. At the community level, a newly trained midwife can pair strong relationships with neighbors with the acquired technical skills to serve as a confidante to local women in a home setting where she can discuss the health issues that matter, accurately describe FP/RH options, and link women and families to standardized care.
With buy-in from village leaders, democratically-run women’s groups are embedded in rural communities and have established themselves as the go-to resource for information on accessing FP/RH services and health information. Many women and families seek advice from a local women’s group before visiting a community health center — testament to their trust. These groups serve as a critical entry point to broader health services, and it is essential that they are engaged in the broader health system, ideally through formal mechanisms such as community health worker (CHW) programs or regular meetings with community health centers.
In many cases, donor-funded activities provide the women’s groups with formal training in behavior change communications to achieve various health and development outcomes. In Mali, trained women’s groups sensitize communities, including men and husbands, on the importance of FP/RH access, empower women of reproductive age to advocate for their own health needs, and build capacity on sustaining these efforts beyond donor-funded activities.
Bridging the Gap between Communities and Health Systems
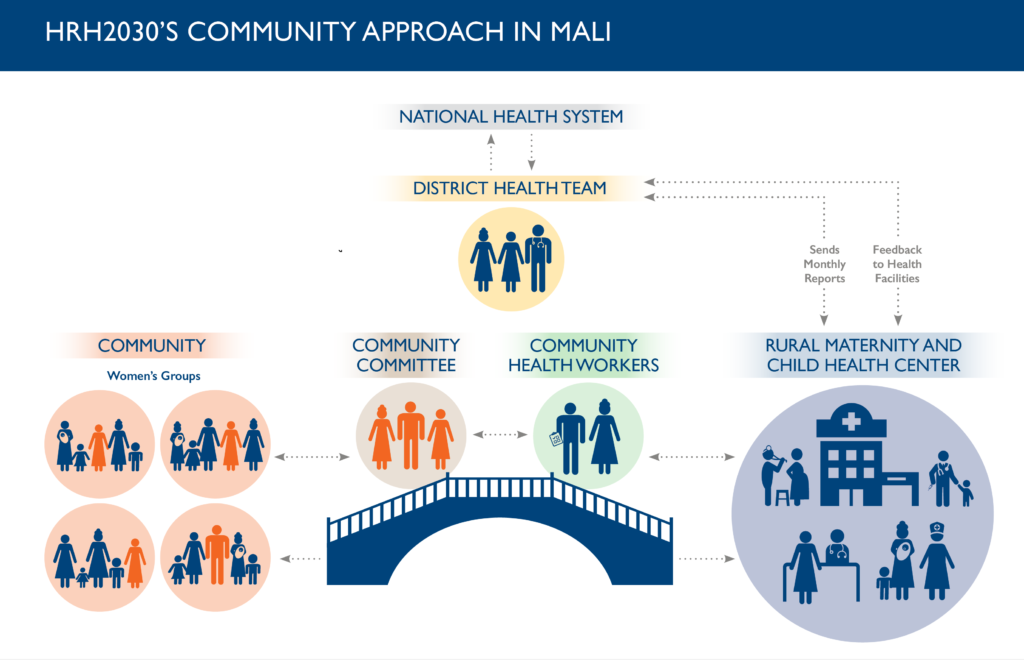
Building the capacity of locally led women’s groups and connecting them to the national health system is an example of how to build a sustainable model that magnifies the work of women’s groups. In the Koulikoro region, and throughout Mali, access to FP/RH services is improving because local and national resources are being simultaneously leveraged. Women’s groups can bridge the gaps between communities and health systems, playing an essential role in Mali’s journey to self-reliance.
As part of USAID’s new policy framework that prioritizes locally driven and sustainable results, the USAID HRH2030 program is connecting women’s groups in Mali to the public health sector at a national level to increase access to essential FP/RH services and support local communities by building the capacity of women’s groups to take charge of their health needs.
The HRH2030 model focuses on enhancing and empowering existing networks rather than creating parallel systems by tapping into women’s groups’ existing networks, which simultaneously fortifies the existing health system and builds the capacity of local actors in Mali. The program works primarily with CHWs, who orient and monitor the women’s groups to ensure they follow national standards and that the program follows contextually appropriate practices. In addition, HRH2030 trains CHWs on FP/RH modules that the CHWs then use to train the women’s groups and then tracks progress through monthly follow-ups. The results during and after the HRH2030 community approach have been impressive: Over an eight-month period, the number of families using an FP/RH method quadrupled across 10 districts.
I concluded that the success of women’s groups is a result of strong individuals harnessing community ties to promote FP/RH access and education combined with an impressive network of dedicated women supporting each other. Donor-funded programs and approaches, such as the community approach used by HRH2030, standardize critical and life-saving activities, promote quality control in measuring results, and provide the resources to expand the groups’ reach.
While donor-funded activities certainly provide necessary support to the women’s groups, they are not a standalone solution. The success of these groups highlights the power of working at the community level, an approach that increases local resilience and catalyzes a country’s journey to self-reliance. Other countries can follow Mali’s lead by empowering and training rural women’s groups, bridging the access gaps that they encounter, and promoting locally led efforts that are more likely to remain in place long after donor-funded activities end.
Posts on the blog represent the views of the authors and do not necessarily represent the views of Chemonics.