Making The Most of It: Optimizing Human Resources for Health for Family Planning
October 10, 2023 | 4 Minute ReadHuman resources for health (HRH) refer to the diverse collective of health workers that drive, manage, and lead health systems. They are doctors, nurses, midwives, community health workers (CHWs), and social workers, but also pharmacists, shop owners, health managers, and educators. This workforce provides health services in various settings, such as hospitals, clinics, offices, virtual spaces, communities, and homes.
To deliver effective healthcare – especially essential primary health care services during public health emergencies – it is important for health facilities, national HRH planners, and implementing partners to use HRH data to configure their health workforce and services in an optimal way. And why does this matter? Because optimizing available HRH means teams are available and ready, which is crucial for improving health outcomes and responding to dynamic global health security challenges, such as those caused by climate change and global pandemics.
Developed by the Chemonics-led USAID HRH2030 Program, the HRH Optimization Tools can support data-driven, locally informed health workforce solutions across contexts by providing users with models and scenarios for task-sharing between cadres as well as service delivery differentiation. By consolidating HRH and service delivery data, these simple, Excel-based tools can identify and address HRH bottlenecks at frontline facilities and provide managers with potential opportunities to increase HRH efficiencies, so health workforce workloads are balanced, and more services are available where people need them.
HRH Optimization for Family Planning
Family planning is a service area where HRH optimization is needed. With a global population that is rapidly growing, ensuring access to high-quality voluntary family planning is crucial. Family planning providers deliver services throughout all areas of health care: hospitals, clinics, offices, markets, and communities. Their geographic distribution, however, can lead to disparities between urban and rural users, high- and low-income users, and by demographics due to economic, social, and cultural factors.
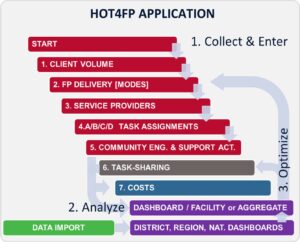
The HRH Optimization Tool for Family Planning helps identify and correct HRH imbalances to promote client-centered family planning services. Within voluntary family planning services, sharing tasks within the workforce in accordance with health workers’ appropriate scope and skill levels can expand service availability, especially for underserved communities. By inputting demographic data, health survey data, and private sector and mobile outreach data to understand who is delivering family planning, where, and via what proportion of FP methods, HOT4FP considers scenarios to meet current and potential client volume and takes environmental, economic, cultural, and social considerations into account to support context-informed and data-driven decision making. For example, if more CHWs provide competent counseling and distribute oral contraceptives at community clinics (where authorized by national policy), then doctors and nurses may have more time to provide family planning services that require higher-level skills, such as inserting implants and IUDs.
How to Use HOT4FP
Questions that national and subnational health leaders could consider when thinking about optimizing their HRH to improve health outcomes across populations, global health security, and the economic growth of a population include:
- Do we have enough health workers, and are they the right kind to meet community needs?
- Are they adequately trained to do their jobs? Are they adequately distributed? Can they adapt when needed in response to emergencies or workforce gaps?
- Do they provide high-quality care?
The HRH2030 Program supported health leaders in Mali’s Dioila district to use HOT4FP and consider similar workforce questions. District managers reviewed current task allocations to understand that within Dioila district, CHWs at health centers had the most time available to take on additional FP tasks, whereas midwives had the least. HOT4FP provides models for district managers to consider what proportion of family planning community education tasks could be shifted from midwives to trained CHWs.
Using optimization tools like HOT4FP, health facilities can use their specific HRH data results to modify and shift focus and resources through task-sharing and expanding service delivery beyond facility walls. For example, in Pakistan where many rural families seek care from Hakeems—traditional medicine practitioners—expanding the role that Hakeems play to provide voluntary family planning counseling could lessen the burden of other CHWs to who are providing additional services to their communities.
HOT4FP data can also help build health system resilience as managers can review scenarios to prepare for public health emergencies and global pandemics. When a health system faces stresses or shocks, such as the COVID-19 pandemic or an environmental disaster, family planning providers must adjust to meet dynamic service demands and ensure high-quality FP services remain available to all.
In 2020, the Mali HRH2030 regional health teams mobilized all coaches and technical staff to focus on COVID-19. Team members adapted family planning activities and put strategies in place to respond to the pandemic’s rapidly evolving context, i.e., sharing CHW guidelines on COVID-19 prevention to help districts integrate COVID-19 messaging into their regular FP communication activities. Implementing these strategies ensured HRH2030 maintained the expected level of community results.
Interested in other HRH tools? You’re in luck! The HRH2030 Program also developed the HRH Optimization Tools for Antiretroviral Therapy (HOT4ART) and Primary Health Care (HOT4PHC), to strengthen the health workforce to meet client demand for services and scale innovative opportunities to deliver care.

About Rachel Deussom
Rachel Deussom is the director of the Chemonics Global Health Practice, with over 17 years of experience focusing on health systems strengthening, human resources for health, community health, digital Health, HIV/AIDS, and maternal and child health. Previously, she acted as the technical director of HRH2030 Program, USAID’s global health workforce flagship project, led by Chemonics.…