Reflection on APHA 2015: Preparing Health Systems for Policy Change
November 5, 2015 | 4 Minute ReadAn analyst tests pharmaceuticals at Kenya's National Quality Control Laboratory. Chemonics presented on its capacity building in Kenya and other countries at this year's APHA conference.
The theme of this year’s American Public Health Association (APHA) Annual Meeting, hosted in Chicago, was “Health in All Policies” (HiAP). This theme emphasized the need for policymakers in all sectors to recognize that environments where we live, work, and attend school have serious implications on health outcomes.
Julián Castro, the U.S. Secretary of Housing and Urban Development, spoke movingly on this topic when recounting the moment when, as mayor of San Antonio, he realized the impact that safe, walkable streets and sidewalks could have on the health of a community. During the same discussion, the U.S. Surgeon General, Dr. Vivek Murthy, called health “the river that runs through everything.” We have seen this concept mirrored in headlines in the U.S. ranging from safety on college campuses to public and legislative debates around gun control.
Policy Change and Capacity Building Go Hand-in-Hand
To be truly effective, health-related policy across sectors should be evidence-based, incorporating best practices based on high-quality data collection, analysis, and evaluation. Yet even policy changes that are driven by data and backed by political will are unlikely to lead to positive outcomes unless a country’s health system has the capacity to meet the new demands brought about by the change.
One clear example of policy outstripping capacity from the United States is expanded health insurance access as a result of the Affordable Care Act, which has led to a net of 16.9 million newly insured Americans, most of them Medicaid recipients. With the newly insured expected to utilize the emergency room less and primary care providers more, the next challenge will be securing the capacity of primary care facilities to accommodate the expanded insured population.
Planning for such changes and building capacity to meet new demands should go hand-in-hand with policy change efforts. This year at APHA, capacity building to achieve national policy objectives was at the heart of two of the USAID-funded projects that Chemonics presented.
Case 1: Family Planning in Rwanda
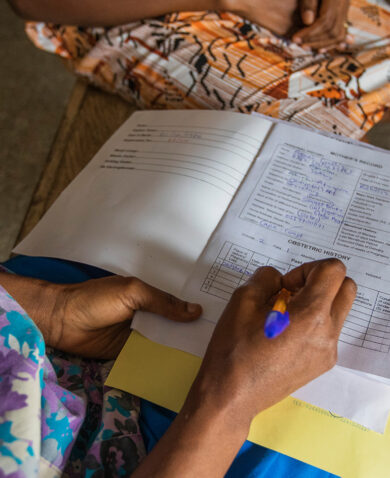
 The Rwandan Ministry of Health has clearly demonstrated a commitment to improving health outcomes through policy. The Ministry of Health is working to increase the demand for family planning methods, espeically long-acting and permanent methods, by integrating services and increasing men’s involvement in family planning discussions. In conjunction with the Ministry of Health, USAID’s Rwanda Family Health Project (RFHP) has achieved measurable results by building the capacity of providers and conducting community-based outreach for family health services.
The Rwandan Ministry of Health has clearly demonstrated a commitment to improving health outcomes through policy. The Ministry of Health is working to increase the demand for family planning methods, espeically long-acting and permanent methods, by integrating services and increasing men’s involvement in family planning discussions. In conjunction with the Ministry of Health, USAID’s Rwanda Family Health Project (RFHP) has achieved measurable results by building the capacity of providers and conducting community-based outreach for family health services.
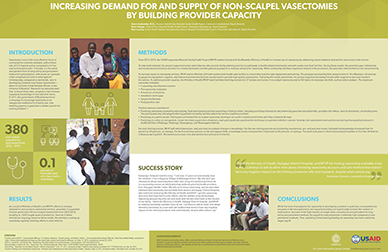
In particular, RFHP collaborated with the Ministry of Health on activities to increase the supply and demand for vasectomies. As a result of activities that included service provider training, mentoring, and coaching, RFHP prepared the health system to meet the increased demand for vasectomies by training 27 doctors and nurses in non-scalpel vasectomies in 14 out of 30 districts. Vasectomy as a family planning method was also incorporated into community health worker training and messaging, and community events provided a forum for men to discuss the benefits of vasectomy on a public stage. While rates of vasectomy in Rwanda were previously close to zero, 380 of the procedures were performed by RFHP-trained providers between 2012 and 2014.
Rwanda’s Ministry of Health now plans to scale up these activities in additional districts. You can read more about this and RFHP’s provider capacity building activities aimed at reducing the burden of obstetric fistula, here and here.
Case 2: Pharmaceutical Supply Chain Management in Kenya
 The Kenyan government is committed to the goal of diagnosing 90 percent of HIV-positive people and treating 90 percent of those diagnosed. With the current HIV prevalence in Kenya, this means providing antiretroviral (ARV) drugs to 1.3 million people.
The Kenyan government is committed to the goal of diagnosing 90 percent of HIV-positive people and treating 90 percent of those diagnosed. With the current HIV prevalence in Kenya, this means providing antiretroviral (ARV) drugs to 1.3 million people.
USAID’s Kenya Pharma project created a secure and sustainable national pharmaceutical supply chain management system to meet policy-driven demand for the care and treatment of persons with HIV/AIDs. Pharma built Kenya’s national capacity to fight HIV/AIDS by building an electronic supply chain management system, providing support to service delivery points, contracting with local medical suppliers for medicines, and engaging with local labs for quality control testing of these drugs. Through its efforts, Pharma achieved remarkable results: zero stock-outs in 2014 (down from 46 percent of service delivery points reporting stock-outs prior to project start-up) while procuring ARVs for more than 386,000 patients.
Overall, Pharma helped ensure Kenya is on the path to achieving the government’s HIV treatment goals. In fact, Pharma’s expansion of treatment availability has been cited as a major contributing factor to reductions in HIV rates in Kenya from 7.2 percent to 5.6 percent over the course of the project. You can view Kenya Pharma’s presentation at this year’s APHA meeting here.
Moving Forward
HiAP is a challenging concept and involves continuous collaborative efforts from a range of stakeholders. By sharing innovations and lessons learned from around the world, both across and within sectors, and getting policymakers onboard with the idea of building capacity to support HiAP, development leaders and communities can work to achieve measurable outcomes in health and beyond.